
How to Spot Vitamin Deficiencies Based on Your Symptoms (Part 3)
A deep dive into vitamins, their functions, and how vitamin therapy may help heal physical and mental conditions

Disclaimer: This content is not intended as treatment or support for any medical condition. Content for entertainment purposes only. Not medical or health advice.
My Substack is a reader-supported publication. The full version of this article is for paid subscribers only.
After the incredible success of part one, I am back with part three of my favourite and highly requested series, this time covering vitamins B4 (choline) and B5.
Part 2: Vitamin D (special spotlight)
If you haven’t yet, I highly recommend that you start by reading the first installment of the series. In “part 1,” you can find the intro to the topic of vitamins, which tells you all about the history of vitamins and why they’re so important. As it turns out, the idea that some (or most) health issues are caused by the deficiency of a vitamin or mineral (or multiple vitamins and minerals) is not at all far-fetched.
Vitamin Deficiencies Are a Silent Epidemic
The idea that a debilitating condition might just be a manifestation of a vitamin deficiency or a vitamin dependency (requiring a supra-physiological dose of a certain vitamin to resolve) is not just a meme. It’s a well-documented phenomenon.
I used to stumble over words and even stutter until I supplemented vitamin B1. I used to have awful ovulation pain until I supplemented vitamin E. I used to have a chronically red nose, and the corners of my lips would often crack until I supplemented vitamin B2. Dry skin and cracked lips? Resolved with more vitamin A. My bleeding gums resolved with vitamin C. My frequent waking stopped being a problem after taking vitamin B8 (inositol), which helps me sleep like a rock. I seldom feel anxious since I started using high-dose magnesium, which also helped me overcome my once common arrhythmia episodes. My uncontrollable cravings for cheese and easy bruising disappeared after taking vitamin K2. My skin rashes disappeared after taking vitamin B7. PMS stopped being a problem once I upped my vitamin C, potassium and vitamin D intake. I also used to be quite emotional, easily depressed and quick to cry. This is no more, since taking selenium, vitamin D, zinc, and increasing my calcium intake.
I want to be clear that I’m not suggesting that vitamin and mineral therapy will fix those same issues for everyone. However, considering that vitamin therapy has the potential to ameliorate health struggles, we really should stop ignoring and undermining it. It should also go without saying that a well-rounded diet should always take precedence before turning to supplement pills, which is why, under every vitamin discussed, there is a section covering dietary sources of said vitamin and how to get enough of it with food alone.
Health is multifaceted and no disease is truly monocausal. However, while we often believe that modern diseases are far more complicated and sophisticated than being the manifestations of subclinical vitamin and mineral deficiencies, this is not always true. With the “branding crisis” that vitamins are currently experiencing, people rarely consider that their depression, ADHD, diabetes, autoimmunity, digestive disorders, hair loss, or PMS might stem from a subclinical vitamin or mineral deficiency (or multiple deficiencies). These symptoms are then treated with medications that may or may not resolve some symptoms. Meanwhile, most of these medications fail to correct the underlying imbalances that are preventing the body from functioning as it should.
The practice of treating various ailments by providing these missing puzzle pieces through correcting underlying vitamin and mineral gaps, including those which may not always overtly flag on tests, is the backbone of orthomolecular medicine. The body of literature on orthomolecular medicine is massive, with medical journals dedicated solely to it, such as the Journal of Orthomolecular Medicine. Unfortunately, this research is often forgotten and taken for granted nowadays, despite how mechanistically sound it is. We know that countless metabolic pathways in the human body have an absolute dependency on vitamins and minerals. It is mechanistically obvious that if the deficits in these pathways are caused by a shortage of the vitamin and mineral cofactors needed to operate them, fixing those gaps will ameliorate those deficits.
Many commonly prescribed medications work on pathways shared with vitamins. For example, some psychiatric medications work in part by blocking glutamate receptors, even though glutamate tends to rise and become dysregulated as a consequence of vitamin B6, magnesium and glycine deficiency. Another example is that of cholinergic drugs, which are meant to mimic acetylcholine at the level of the nervous system. Vitamins B4 and B5 are needed to make acetylcholine. While there is absolutely a time and place for targeted medication, I think it’s safe to say that a more sensible approach would be to first fill in these nutrient gaps before assessing the need to turn to potent pharmaceutical solutions.
The term “orthomolecular” was coined by Linus Pauling, a pioneer of molecular biology and a recipient of multiple Nobel Prizes, including in chemistry. Orthomolecular medicine has been successfully used to treat cases of various psychiatric disorders, degenerative brain disorders, age-related vision loss, all types of skin problems, reproductive problems, and autoimmune disorders.
None of this should be shocking, considering that vitamins and minerals are needed to harness energy from foods, create neurotransmitters, synthesize hormones, repair tissues, and help the body fight off pathogens and rid itself of metabolic and environmental toxins.
Yet, disease symptoms are rarely linked to deficiencies, on the incorrect assumption that vitamin deficiencies are rare. Vitamin deficiencies are not rare. Between refined diets, stress and pollution accelerating vitamin depletion, the poor quality of most nutritional supplements, the lower vitamin and mineral content of animal and plant foods (due to soil depletion and poor animal husbandry), and the shortcomings of most tests geared at testing micronutrient levels, vitamin and mineral deficiencies are an absolute epidemic.
The good news is that, with a bit of self-examination, there are ways to spot specific deficiencies all by yourself. This article series provides you with the tools to answer questions like:
Do I fit the picture of having multiple physical or psychological symptoms specific to the deficiency of a certain vitamin? If I treat the symptom list like a Bingo card, do most of them apply to me?
Do my general lifestyle habits fit the list of habits that put someone at risk of a specific deficiency?
Does my diet make me prone to that deficiency based on what I do (or do not) eat?
Do my past blood tests show that certain bodily vitamin-dependent functions are operating sub-optimally, even if no direct vitamin measurements were flagged as “below range”?
My goal is to help my readers become more self-sufficient in managing their health.
After all, even if the diet is well-rounded, many factors can interfere with the use of nutrients, accelerate their breakdown and depletion, or make someone’s need for a certain nutrient higher than that of an average person, due to underlying genetic or metabolic peculiarities.
Taking a good, hard look at what the body is trying to tell us can be just as (if not more) valuable than comprehensive testing. The “hack” is knowing how to understand the body’s language.
In This Article:
This is the third part of a series diving deep into vitamins, their functions, and how their deficiencies manifest. This article covers: vitamin B4 (choline) and vitamin B5.
The topics covered in this installment can be of particular interest to those afflicted with: fatty liver disease, gallstones, dementia, digestive issues, cholestasis, manic episodes, acne, arthritis, “adrenal fatigue,” hair loss, high homocysteine, low hormone levels, pregnancy-related cognitive decline
Table of Contents:
Vitamin B4 (Choline)
The liver-fat-burning, membrane-building, rest-and-digest cognitive enhancer.
Predominant deficiency symptoms:
chronically dry mouth, fatty liver, gall stones, poor memory (short-term memory, visual memory, spatial memory), lack of mental “sharpness,” impaired digestive motility (feeling full after little food, uncomfortable “fullness” in the stomach, constipation, difficulty swallowing), anxiety, lack of control over facial muscles (drooping, numbness), nicotine cravings, chronic pain, agitation, struggling to digest meat
The Importance of Choline:
“When deprived of dietary choline, 77% of men and 80% of postmenopausal women developed fatty liver or muscle damage.”
- from: Sex and menopausal status influence human dietary requirements for the nutrient choline. (doi: 10.1093/ajcn/85.5.1275)
“Justice for choline!” is what I want to scream from the rooftops after doing my deep dive into this precious vitamin.
Most people don’t even know that there is such a thing as vitamin B4. Poor, poor choline is often forgotten because, if we focus on semantics, it doesn’t precisely fit into the “vitamin” category.
As explained in the first installment of this series, for a compound to be classified as a vitamin, it has to meet two criteria:
It has to be a natural compound necessary for the normal growth, development, and function of a living organism.
It has to be a compound that the body can’t make on its own and must obtain from food.
While choline indisputably meets the first criterion, its membership in the “vitamins club” was initially declined because, technically, the body can create its own choline.
Choline can be indirectly synthesized in the liver through the PEMT pathway. The pathway creates phosphatidylcholine, a major component of our cell membranes, which can later release choline when broken down. However, this pathway is very expensive. If your methylation is impaired and if your liver is struggling, your ability to make choline will be massively thwarted.
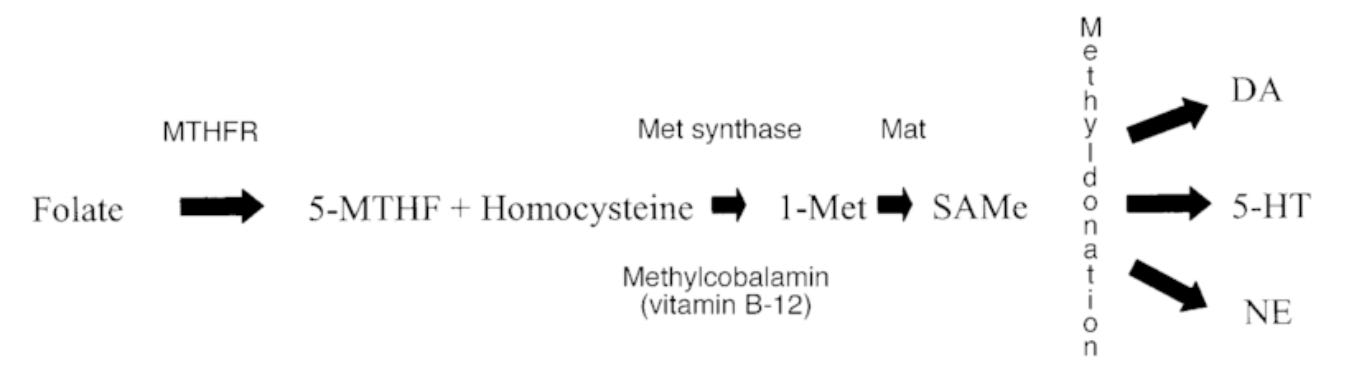
To make its own choline, the body must obtain methyl groups from S-adenosylmethionine (SAM).1 SAM itself is a costly compound. Its creation is dependent on sufficient methionine, folate, vitamin B2, vitamin B6, vitamin B12, adequate function of the MTHFR enzyme, and enough ATP (the energy molecule).23
The biggest kicker to it all? Choline itself is a methyl donor, and its methyl groups help replenish our SAM pool.4
Knowing just how prevalent the deficiencies of these B vitamins are, and that ATP production is slashed in most disease or “unwellness” states, it becomes clear that making its own choline is no easy feat for the body.
In 1998,5 it was finally recognized that the importance of dietary choline has been massively understated, and choline has been re-classified as a “vital amine” (a vitamin) on the observation that, even under ideal conditions of ample ATP, full-throttle liver function, and B-vitamin abundance, the human body only makes a tiny bit of choline and is incapable of making enough to meet its needs.
Considering that choline is vital to maintaining proper liver function in the first place, this re-classification was long overdue.

Animal and human studies show over and over again that insufficient dietary choline leads to fatty liver disease, growth disorders, neurological diseases, digestive disorders, gallstones, cholestasis, muscle damage, and reproductive disorders (including preeclampsia). Choline insufficiency even plays a role in heart disease, kidney disease, and cancer. Animal models show that choline deprivation alone is enough to cause liver cancer, even without exposure to any carcinogens.6 Fatty liver disease is an epidemic, and choline is the primary vitamin that prevents its development.
Still, even though nutritional researchers officially said “sorry” to choline, this vitamin remains forgotten. It also seems that there is some sort of collective amnesia around the 1998 re-classification of choline as a vitamin. Most publications still erroneously claim that choline is not a vitamin!
Choline is often so forgotten that even most B-complex supplements fail to include it in the formulation. The fact that the importance of dietary choline has been understated for so long is a massive disservice to us all.
Choline Protects Against Fatty Liver & Gallbladder Disease

Choline is needed to move fats and cholesterols out of the liver, to keep bile soluble and prevent gallstones, and to promote bile release during digestion.
The term “choline” is derived from “chole,” the Greek word for bile,7 after first being isolated from pig bile in the mid-1800s. That this vitamin is vital to bile flow and gallbladder health should be obvious by its name alone.
We all know that water and oil don’t mix. However, you can mix water and oil by adding an emulsifier. Choline is an emulsifier. Choline is the reason why, when you mix egg yolks with lemon juice and oil, the end result is mayonnaise. Egg yolks provide choline.

Since fats don’t dissolve in water, cholesterol and other fats in your bile need to be emulsified to flow freely. When choline is deficient, the cholesterol in bile hardens, eventually resulting in gallbladder stones.
Choline is a building block of the vLDL lipoprotein that transports fats out of the liver. Without this lipoprotein raft, fats can’t leave the liver. This eventually leads to fatty liver disease, especially in those who are overweight or on high-fat diets, which increases the flux of fat into the liver.
While your cardiologist might be overjoyed if they see that your LDL levels are super low, they don’t consider LDL contextually. If LDL is low because you can’t make enough due to choline deficiency, then you’re on the fast-track towards non-alcoholic fatty liver disease.
In addition to accelerating fat export, choline modulates gene expression in the liver to promote fat burning and stop the synthesis of new fats.8
As early as the 1930s, it was shown that animals deprived of dietary choline develop fatty liver disease.9 The same is true in humans, and choline supplementation has been successfully used to remove liver fat and reverse fatty liver disease caused by its deficiency.10
“Humans eating diets low in choline develop fatty liver and liver damage. Rodents fed choline–methionine-deficient diets not only develop fatty liver, but also progress to develop fibrosis and hepatocarcinoma. […] When humans eat diets low in choline, fatty liver is one of the earliest adverse events.”11
Recently, awareness has been growing around the deleterious effects of mold toxins. Mold toxins aflatoxin B1 and fumonisin B1, which often contaminate corn, induce more liver damage in choline-deficient rodents.1213
Mold toxins can impair the flow of bile out of the liver, contributing to cholestasis (chole = bile, stasis = static, static bile).
Since choline is needed for good bile flow, choline deficiency greatly increases the risk of mold-induced cholestasis. In cholestasis, bile acids start spilling into the blood, where they can damage the kidneys and other organs.14 Extra choline is protective in this scenario.
Apart from choline deficiency, bacterial toxins produced by bad gut bacteria, such as endotoxin, are a major contributor to fatty liver disease.15 When the microbiome is overgrown or dysbiotic, the diet lacks protective plant compounds, and the gut lining is injured, toxins produced by bad gut bacteria can leak from the gut to the liver.
The gut lining becomes injured (a phenomenon typically referred to as “leaky gut”) in states of stress, malnutrition, low metabolism, alcohol consumption, or Candida infections, since Candida produces the same toxins that alcohol breaks down into.16 (A person with a bad case of Candida becomes “perpetually hungover.”)
Endotoxin is highly inflammatory, and once it reaches the liver, it kicks off a massive immune response, as the liver scrambles to get rid of it. Since endotoxin can directly “suffocate” mitochondria and block the “pipeline” that turns food into energy, an endotoxin-stricken liver struggles to burn fuel and deposits it as fat instead. The increased production of fat in the liver may also be a protective mechanism, since fat can trap and inactivate endotoxin. However, chronic, unopposed exposure to bacterial endotoxin eventually leads to fatty liver disease.
Choline, as phosphatidylcholine, is needed to make the HDL lipoprotein (the so-called “good” cholesterol). HDL and LDL both help trap and inactivate endotoxin, so that it doesn’t reach and damage the liver. Between the two, HDL is the primary front of defence.17 The phosphatidylcholine portion of HDL and LDL is what’s specifically responsible for trapping and neutralizing endotoxin. In rats injected with a lethal dose of endotoxin, a high-choline diet completely prevented mortality.18 The most likely explanation is that a high-choline diet increased the synthesis of lipoproteins that can bind, restrain, and neutralize endotoxin in the blood.
In summary, choline protects against fatty liver disease in several direct and indirect ways.
Choline Controls Every Part of Digestion
Choline is a building block for acetylcholine, the rest-and-digest neurotransmitter that’s released when the vagus nerve is activated.
You can do all the relaxation techniques to try and stimulate the vagus nerve before meals for improved digestion, but they’ll have little effect if choline is seriously deficient.
My Substack is a reader-supported publication. You can support my writing and independent research efforts by becoming a paid subscriber. Monthly subscriptions are $15 per month, and can be cancelled at any time. You save with a yearly subscription, as $100 grants you access to my full archive for a year.
Unlock the full version of this article by becoming a paid subscriber.